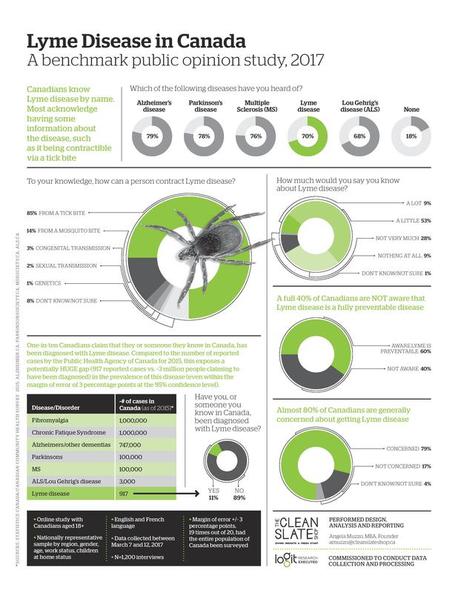
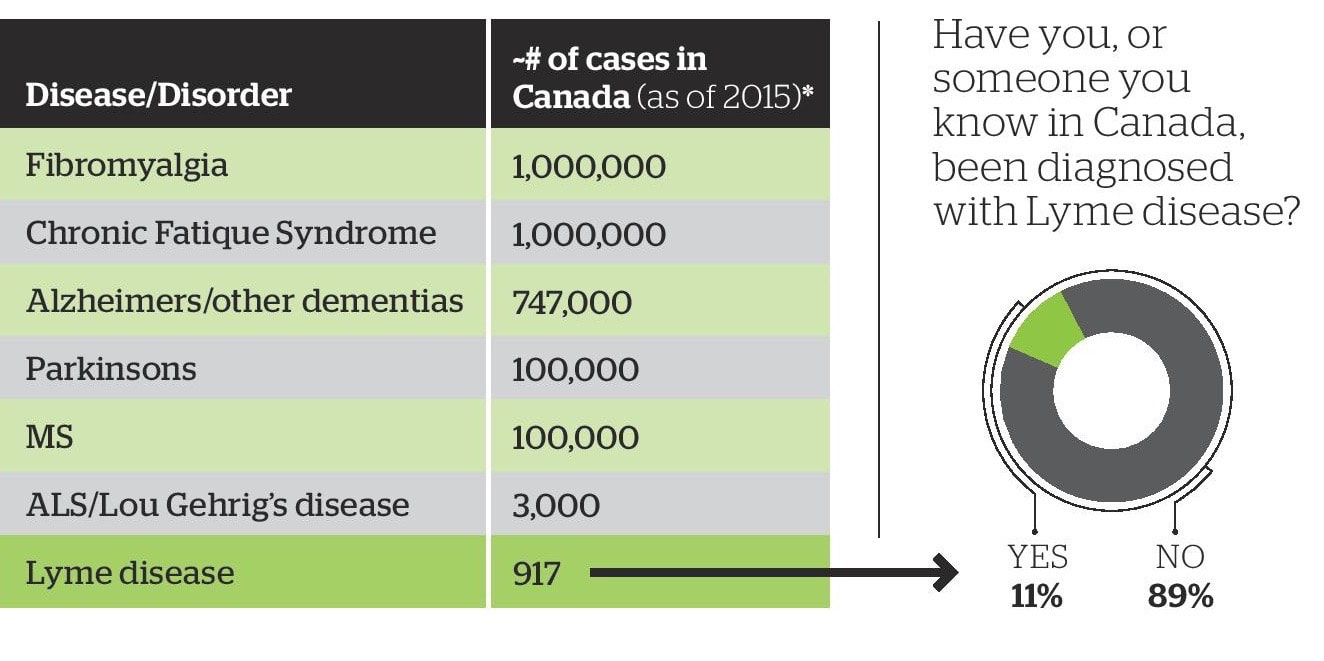
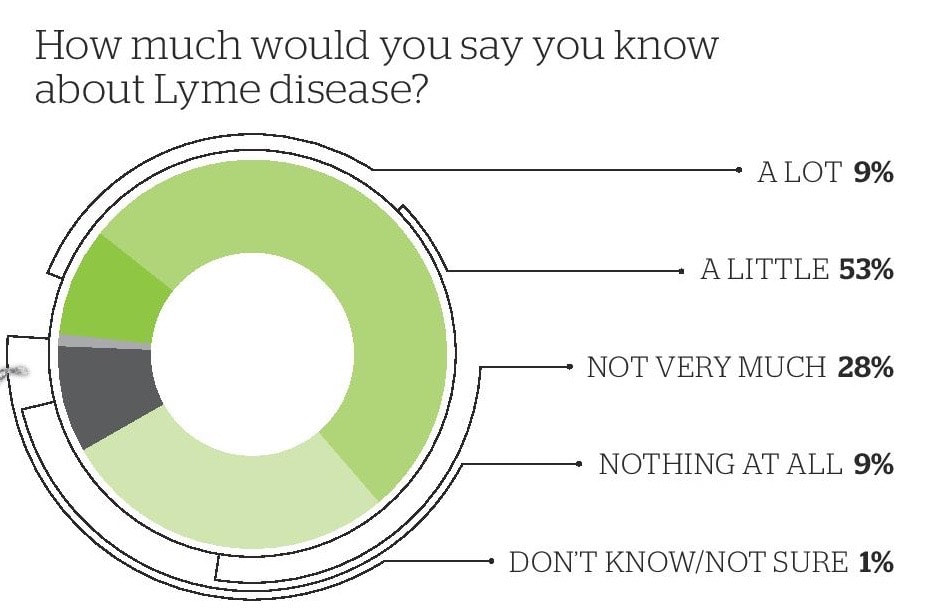
 Findings include: Approximately 4 million Canadians report that they or someone they know in Canada has been diagnosed with Lyme disease. Compared to the number of reported cases by the Public Health Agency of Canada for 2015 of 917 cases.
0 Comments
 Copyright: vladone / 123RF Stock Photo Action: Please Invite Your MP to Attend a Federal MP Round Table on Lyme Disease (May 7th)On Monday May 7th, Ms. Tracey Ramsey, M.P. (NDP, Essex, Ontario) and Mr. Randy Hoback, M.P (Conservative, Prince Albert Saskatchewan) in partnership with LymeHope, CanLyme, the G. Magnotta Foundation for Vector-Borne Diseases and Provincial Lyme groups, is hosting an educational round table event on Lyme Disease in Ottawa.
This event is for Federal MPs only (not for members of the public). This is a non-partisan initiative (open to all political parties). We hope to see as many MPs as possible in attendance, so that they can hear first-hand the seriousness of this rapidly growing health threat. MPs are responsive to the needs of their constituents, so we need your help to reach out to your federal MP and ask them to attend. Action: 1. Click on the link below to find your federal MP by entering your home town or postal code. Your MP will show up and you can click on their name to get an email and office telephone numbers. https://www.ourcommons.ca/parliamentarians/en/constituencies/FindMP 2. Copy and paste the agenda below into a personal email to your MP, tell them you are very concerned about Lyme disease and ask them to attend. 3. Follow up with a personal phone call to their Constituency and Ottawa office and ask your MP’s assistant to ensure this invitation is brought to their attention and the importance that they attend on your behalf. We will be in attendance at this round table and will provide a comprehensive update afterwards. Thank you for your continued support. With Hope, Jennifer Kravis & Sue Faber Co-Founders LymeHope www.lymehope.ca Ms. Tracey Ramsey, M.P. & Mr. Randy Hoback, M.P. in partnership with LymeHope and CanLyme and G. Magnotta Foundation welcome you to an MP Round Table: “Lyme Disease across Canada” Details: Monday May 7th, 2018, 5:30pm – 6:30pm Room 310, Wellington Building, Ottawa, Ontario This event is also supported by the following organizations: New Brunswick Lyme Disease Association Inc ./ Association néo-brunswickoise de la maladie de Lyme inc. (LymeNB) l’Association québécoise de la maladie de Lyme (AQML) Nova Scotia Lyme Support Group Vocal Ottawa Ontario Lyme Alliance Lyme Ontario Lyme Disease Association of Alberta (LDAA) Saskatchewan Lyme Disease Association (SLDA) Agenda: Introduction & Welcome Ms. Tracey Ramsey, M.P. and Randy Hoback M.P. Sue Faber and Jennifer Kravis, LymeHope Jim Wilson, President, CanLyme Rosanna Magnotta, G. Magnotta Foundation Dr. Melanie Wills, PhD Director, G. Magnotta Lyme Disease Research Lab, University of Guelph A Scientist's Perspective: Lyme Disease in Canada Daniel Stimers, age 11, founder of the L.E.T. (Lyme Education Team) – elementary students raising awareness of Lyme disease Dr. Ralph Hawkins MD, LLM, FRCPC Clinical Associate Professor, University of Calgary, Site Lead for General Internal Medicine at the Calgary South Health Campus and Plenary Speaker at Public Health Agency of Canada sponsored Framework on Lyme Disease Conference A Physician's Perspective: Diagnosing Lyme Disease in Canada: How the status quo fails the majority Dr. Adrian Baranchuk MD, FACC, FRCPC, FCCS Professor, Medicine, Queen’s University President, International Society of Electrocardiology Editor-in-Chief, Journal of Electrocardiology Vice-President (Canada), Inter-American Society of Cardiology (IASC) A Physician’s Perspective: Lyme Carditis & the electrical system of the heart Sue Faber RN, BScN Co-Founder LymeHope A Nurse's Perspective: Patient First Treatment of Lyme Disease. Registered Nurses Association of Ontario Resolution on Lyme Disease Emma Smashnuk, age 14, Lyme sufferer and advocate. Founder of Emma’s Lyme Ribbon Campaign. Patient and Family Perspective Jennifer Kravis & Sue Faber Co-Founders of LymeHope Wrap Up and Next Steps Q&A  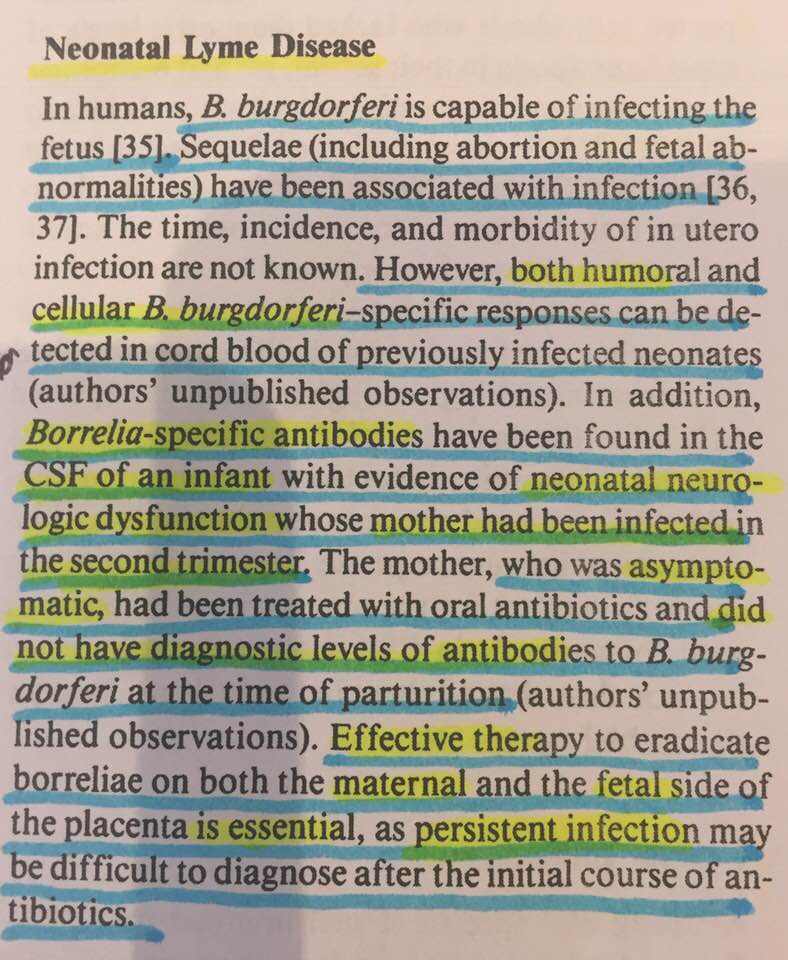 Informative Case Study on Congenital Transmission of Lyme Found in: Dattwyler R, Volkman D and Luft B. Immunologic aspects of Lyme borreliosis. Review of Infectious Diseases Vol 11(6), 1989. 'In humans, B burgdorferi (Lyme) is capable of infecting the fetus. Sequelae (including abortion and fetal abnormalities) have been associated with infection. Borrelia-specific antibodies have been found in the CSF of an infant with evidence of neonatal neurologic dysfunction whose mother had been infected in the second trimester. The mother who was asymptomatic, had been treated with oral antibiotics and did not have diagnostic levels of antibodies to B burgdorferi at the time of parturition (authors’ unpublished observations). Effective therapy to eradicate borreliae on both the maternal and the fetal side of the placenta is essential, as persistent infection may be difficult to diagnosed after the initial course of antibiotics." This little case certainly has important teaching points and big implications: 1: The mom was asymptomatic but followed by researchers because she was infected (presumably with a tick bite) in her second trimester 2: Researchers were interested in the outcome and followed her pregnancy. 3: Mom was TREATED with oral antibiotics 4: At time of giving birth - Mom is SERONEGATIVE by standard testing - meaning she would not be positive on standard lyme tests. 5: Early, but noncurative, treatment was presumably felt the explanation for her seronegativity 6: Baby is born with neonatal neurologic dysfunction 7: A spinal tap on neonate reveals serological evidence of antibodies specific to borrelia in cerebral spinal fluid. 8: This is a congenitally infected baby. Borrelia burgdorferi has been transmitted from asymptomatic mom who was inadequately treated and seronegative - to her baby. 9: Authors go on to EMPHASIZE the importance of effective therapy to erradicate borreliae on both maternal and fetal side of the placenta - as PERSISTENT infection may be difficult to be diagnosed after the initial course of antibiotics . 10: Authors one-line recommendation based on this case has huge potential ramifications for management of pregnant moms infected with Lyme and their infants.  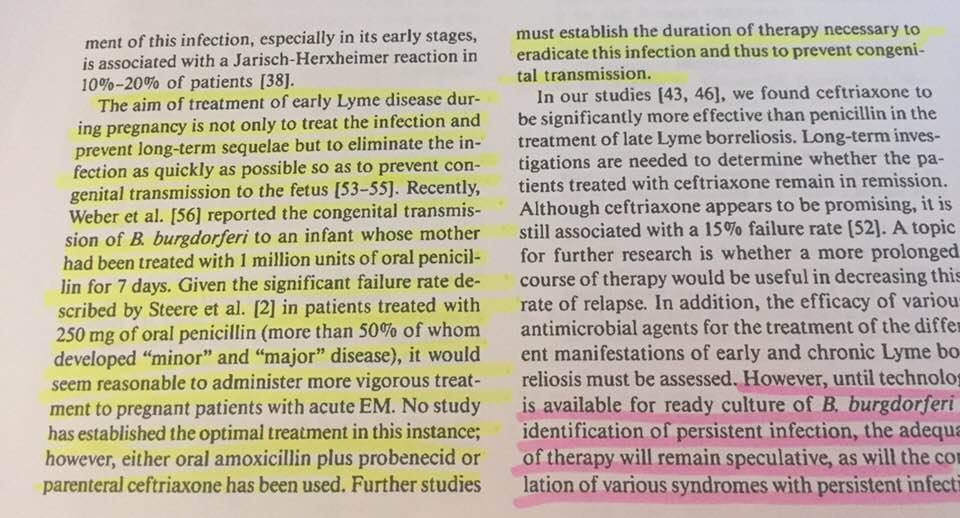 In a separate paper (above) in the same top-tier journal by the same authors, with an addition of Dr. Gorevic: Luft B, Gorevic P, Halperin J, Volkman D, Dattwyler R. A Perspective on the Treatment of Lyme Borreliosis. Review of Infectious Diseases Vol 11(6), 1989. Authors state: "The aim of treatment of early Lyme disease during pregnancy is not only to treat the infection and prevent long-term sequalae but to eliminate the infection as quickly as possible so as to prevent congenital transmission to the fetus. Recently Weber et al. reported the congenital transmission of B burgdorferi to an infant whose mother was treated with 1 million units of oral penicillin for 7 days. Given the significant treatment failure rate described by Steere et al in patients treated with 250mg of oral penicillin (more than 50% who developed 'minor' and 'major' disease). it would seem reasonable to administer more vigorous treatment to pregnant patients with acute EM. No study has established the optimal treatment in this instance; however either oral amoxicillin plus probenicid or parenteral ceftriaxone has been used. Further studies must establish the duration of therapy necessary to eradicate the infection and thus to prevent congenital transmission." *** Authors in this paper are concerned because congenital transmission IS happening/has been reported and they want to PREVENT congenital transmission and so they are questioning what the appropriate antibiotic therapy should be. This is not a question of it's 'plausible' or 'theoretically possible' that this alternate mode of transmission occurs. It IS happening. It has been PROVEN. 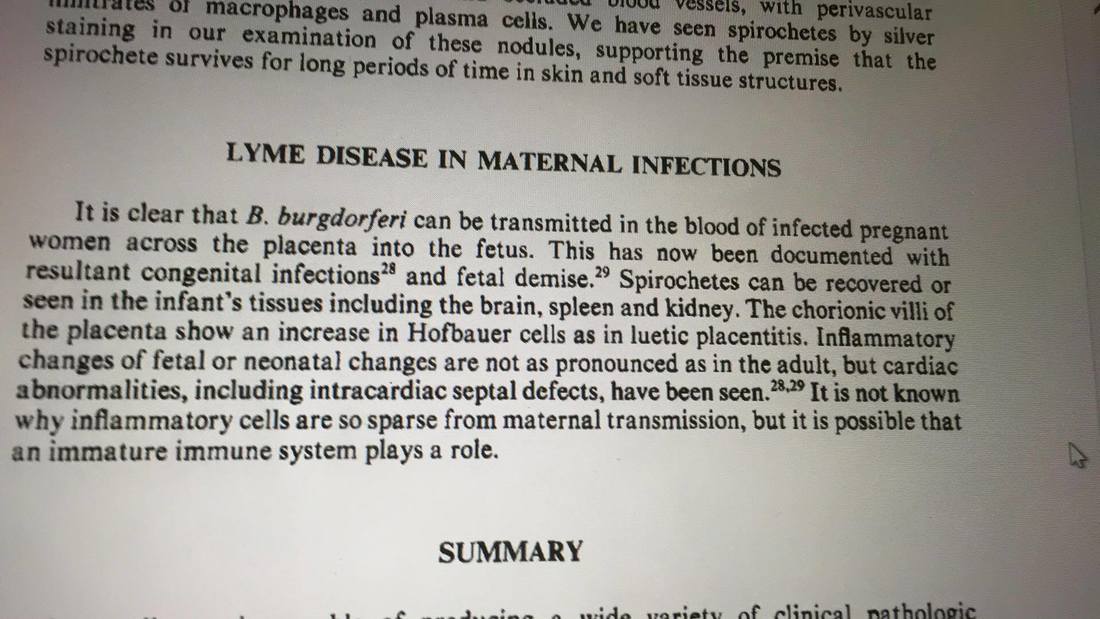 The excerpt and picture above is from a top-tier, world renowned, medical journal and authored by medical doctors and researchers. Title: Clinical Pathologic Correlations of Lyme Disease by Stage Authors: Duray, P. and Steere, Alan, C. 1988. Annals of the New York Academy of Science Vol: 539:65-79 Correspondence: PAUL H. DURAY Department of Pathology Fox Chase Cancer Center Philadelphia, Pennsylvania ALLEN C. STEERE Department of Internal Medicine Division of Rheumatology Tufts University School of Medicine Boston, Massachusetts 02111. These authors were/are the leading Infectious Diseases Society of America (IDSA) researchers - they also worked with the Centers for Disease Control. 'It is clear that B. Burgdorferi can be transmitted in the blood of infected pregnant women across the placenta into the fetus. This has now been documented with resultant congenital infections and fetal demise. Spirochetes can be recovered or seen in infant's tissues including the brain, spleen and kidney. The chorionic villi of the placenta show and increase in Hofbauer cells as in luetic placentitis. Inflammatory changes of fetal or neonatal changes are not as pronounced as in the adult, but cardiac abnormalities, including intracardiac septal defects, have been seen. It is not known why inflammatory cells are so sparse from maternal transmisson but it is possible that an immature immune system plays a role.' So what does this mean?How many babies are being missed..who have a congenital infection with Borrelia burgdorferi causing their neurological condition or other symptoms, that, if identified and treated, could get better and indeed have quality of life? We have no idea because most physicians aren't aware and we aren't even looking and this alternate mode of transmission is not acknowledged. It's not just ticks. Borrelia burgdorferi can also be transmitted in-utero without a child ever having a tick bite. This has been repeatedly documented in case-reports and case series. This makes sense considering all the other TORCHES infections can be transmitted in utero resulting in congenital infection and serious sequalae. Lyme is no different. In fact, in the current 2016 edition of Remington and Klein Infectious Diseases of the Fetus and Newborn Infant, In Chapter 1, Current Concepts of Infections of the Fetus and Newborn Infant, authors state this: 'A new acronym is needed to include other, well-described causes of in-utero infection: syphilis enteroviruses varicella zoster virus HIV Lyme disease (Borrelia burgdorferi) Parvovirus Plasmodium and Trypanosoma cruzi (Chagas Disease) Authors propose the inclusive acronym TORCHES CLAP In Table 1-4 - authors review Suggested Acronym for Microorganisms responsible for Infection of the Fetus In Table 1-5 - authors identify Borrelia burgdorferi as causing congenital disease. Maldonato, Y, Nizet, V, Klein, J, Remington, J, Wilson, C. Current concepts of Infections of the Fetus and Newborn Infant. Chapter 1. page 6. Infectious Diseases of the Fetus and Newborn Infant. 8th Edition. 2016 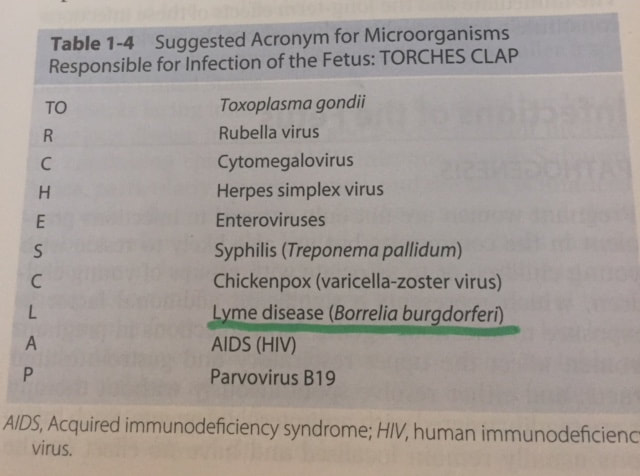 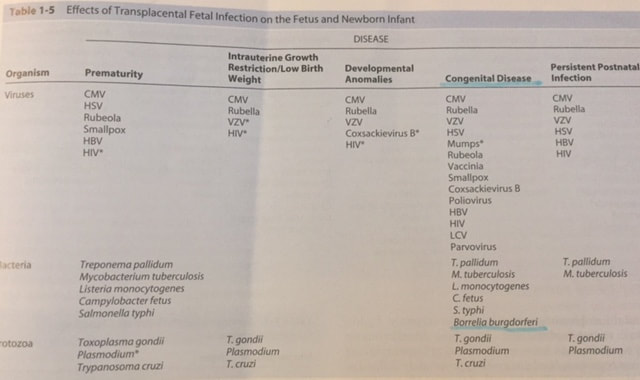 This REALITY and EXISTENCE of maternal child transmission of Borrelia burgdorferi (Lyme) has been reported, discussed, published and AGREED upon by early pioneers in Lyme research and International clinicians and scientists - for direct quotes from these authors please review this document which I compiled and posted to LymeHope:
http://www.lymehope.ca/advocacy-updates/march-03rd-2018 Below are some of the names of some of these physicians, researchers and scientists who published or reported on various aspects of maternal child transmission and or congenital Lyme borreliosis. This is an incomplete list. 1: Dr Willy Burgdorferi (deceased) - discovered the bacterial pathogen that causes Lyme disease, a spirochete named Borrelia burgdorferi in his honor 2: Dr Alan Steere - Professor of Medicine, Harvard Medical School, Member of Infectious Disease Society of America (IDSA) 3: Dr Paul Duray (deceased) - Pathologist, American Society of Clinical Pathologists, Flight Surgeon 4: Dr Alan Barbour - Professor of Medicine and Microbiology & Molecular Genetics, School of Medicine, UC Irvine 6: Dr Raymond Dattwyler - Immunologist, Internal Medicine. Professor of Microbiology and Immunology - New York Medical College. 7: Dr David Volkman - Emeritus Professor of Medicine and Pediatrics SUNY, Stonybrook . 8: Dr Benjamin Luft - Infectious Disease School of Medicine, Stony Brook 9: Dr Peter Schlesinger - Department of Medicine, Hennepin County Medical Center, University of Minnesota Medical School 10: Dr Barbara Burke 11: Dr Thomas Stillman -Rheumatology specialist in Minneapolis, MN 12: Dr Alan Macdonald - Internal Medicine and Pathologist 13: Dr Paul Lavoie (deceased) - Clinical Professor of Medicine at UCSF, Founding Fellow of the American Rheumatology Association 14: Dr B. P. Lattner 15: Dr S E Malawista (deceased) - Professor of medicine within the rheumatology department of Yale University. Malawista is credited as the co-discover of Lyme disease and led the research team which identified the disease 16: Dr R.C Johnson . 16: Dr Jorge Benach - Pathologist, Chairman of the Department of Molecular Genetics and Microbiology, Stony Brook School of Medicine. Dr. Benach has made an indelible mark on science, including his identification of the etiologic agent of Lyme disease 17: Dr. Klaus Weber MD, Dermatologist in private practice, Germany, trained at Harvard. 18: Dr Hans-Jurgen Bratzke -Department of Legal Medicine at the University of Frankfurt 19: Dr Uwe Neubert 20: Dr Bettina Wilske -Max von Pettenkofer-Institute, University of Munich, National Reference Centre for Borreliae, Munich, Germany 22: Dr Tessa Gardner - Infectious Disease Paediatrician. Trained at Harvard University. Author of Chapter 11 on Lyme disease as found in reference textbook - Remington and Klein's Infectious Diseases of the Fetus and Newborn Infant. 23: Dr John Drulle MD - (deceased) 24: Dr Charles Ray Jones - Pediatrician treating congenital Lyme cases 25: Dr Giusto Trevison - Institute of Dermatology and Institute of Microbiology, University of Trieste, Trieste, Italy 26: Dr Giuseppe Stinco - Institute of Dermatology and Institute of Microbiology, University of Trieste, Trieste, Italy 27: Dr Marina Cinco - Institute of Dermatology and Institute of Microbiology, University of Trieste, Trieste, Italy 28: Dr W.T Harvey (deceased) Former NASA physician and epidemiologist 29: Dr P. Salvato- Internal Medicine 30: Dr Gulzade Unk (Department of Pediatrics Faculty of Medicine, Zonguldak Karaelmas University, Turkey) 31: Dr Ceyda Acun (Department of Pediatrics Faculty of Medicine, Zonguldak Karaelmas University, Turkey) 32: Dr Murat Kalaycf (Department of Neurosurgery, Faculty of Medicine, Zonguldak Karaelmas University, Turkey) 33: Dr Ferda Cagave (Department of Neurosurgery, Faculty of Medicine, Zonguldak Karaelmas University, Turkey) 34: Dr Bektas Acikguz (Department of Obstetrics and Gynecology, Faculty of Medicine, Zonguldak Karaelmas University, Turkey) 35: Dr H. Tanriverdi (Department of Obstetrics and Gynecology, Faculty of Medicine, Zonguldak Karaelmas University, Turkey) 36: Dr Harold Smith - MD, Emergency Medicine, Member of ILADS 37: Dr L. V Elsukova - Department of Obstetrics and Gynecology, Perm State Medical Institute. Gamaleya Research Institute of Epidemiology and Microbiology of the Russian Academy of Medical Sciences. (Russia) 38: Dr E. I Korenberg - Department of Obstetrics and Gynecology, Perm State Medical Institute. Gamaleya Research Institute of Epidemiology and Microbiology of the Russian Academy of Medical Sciences. (Russia) 39: Dr G. A. Kozin - Department of Obstetrics and Gynecology, Perm State Medical Institute. Gamaleya Research Institute of Epidemiology and Microbiology of the Russian Academy of Medical Sciences. (Russia) 40: Dr Vera Maraspin - Department of Infectious Diseases, University Medical Centre, Ljubljana, Slovenia. 41: Dr J. Cimperman - Department of Infectious Diseases, University Medical Centre, Ljubljana, Slovenia. 42: Dr Lotric-Furlan - Department of Infectious Diseases, University Medical Centre, Ljubljana, Slovenia. 43: Dr Pleterski-Rigler - Department of Infectious Diseases, University Medical Centre, Ljubljana, Slovenia. 44: Dr Frank Strle - Department of Infectious Diseases, University Medical Centre, Ljubljana, Slovenia. 45: Dr. T. L. Lazebnik - St. Petersburg Medical Academy of Postgraduate Education, St. Petersburg, Russia 46: Dr P. L. Zal’tsman - St. Petersburg Medical Academy of Postgraduate Education, St. Petersburg, Russia 47: Dr James M O’Brien, Division of Maternal Fetal Medicine, Pennsylvania College of Medicine, USA 48: Dr Odessa P Hamidi, Department of Obstetrics and Gynecology, Pennsylvania College of Medicine Are you concerned by this as we are? Sign, comment and share our Lyme Petition. https://www.change.org/p/minister-petitpas-taylor-ticking-lyme-bomb-in-canada-fix-canada-s-lyme-action-plan-now 'Beacon of Hope, Anchored in Integrity' www.lymehope.ca  Copyright: sifotography / 123RF Stock Photo Action Requested: Ontario Government Seeking Comments on Draft Lyme Educational Materials: The Ontario government has issued 2 draft educational materials on Lyme disease - they are calling for public input on the materials until midnight Monday, April 16th. Your feedback is needed and appreciated. You do not need to live in Ontario to participate. The documents and the online feedback form can be found here: https://www.surveygizmo.com/s3/4264305/Lyme-Disease-Guidance-Documents-Feedback-Survey Concerns with Clinical Guidance Document: The biggest concern with the Clinical Guidance document (the flow chart) is that it reinforces many of the “Lyme myths” and is not equipping physicians to properly recognize, diagnose and treat Lyme disease and Co-Infections. There are numerous issues, but some of the most serious flaws are:
Furthermore, the most up to date treatment guidelines (2014) for Lyme disease published by the International Lyme & Associated Diseases Society (ILADS) state: “The potential harms of the single-dose oral doxycycline prophylactic regimen and the magnitude of those harms significantly outweigh its benefits”, and “Clinicians should not use a single 200 mg dose of doxycycline for Lyme disease prophylaxis.” (ILADS Guidelines, Recommendation 1a).
Click below to read why Dr. Elizabeth Maloney and Dr. Daniel Cameron, who both have diagnosed and treated hundreds of Lyme patients, recommend against the single-dose strategy.
Dr David Volkman, Ph.D., M.D. Emeritus Professor of Medicine and Pediatrics SUNY, Stony Brook, NY Background: Board certified in Immunology, Diagnostic Laboratory Immunology, and Internal Medicine, and Board Eligible in Infectious Diseases - speaks to his concerns about the single dose doxy and other issues in a paper he wrote several years ago - these concerns remain relevant today.
Concerns with Public Fact Sheet: Some of the concerns with the Public Fact Sheet:
 Patients, family members, friends, and human/animal health care providers – everyone from any country – is encouraged to comment! Your feedback is needed to change the way physicians treat Lyme disease and to ensure the public is properly informed! Please share and share again! You can also share feedback by participating in a virtual Town Hall Meeting which will be set up by the Government of Ontario – details will be shared as they become available. Thank you as always for your continued engagement and support. Jennifer Kravis, BA, LL.B & Sue Faber, BScN, RN Co-Founders LymeHope |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
September 2020
Categories |
||||||||||||
 RSS Feed
RSS Feed